Six Months Against COVID-19
Six months ago, President Joko “Jokowi” Widodo seemed to be racing against time, announcing the first two cases that were confirmed to be infected with the virus that causes COVID-19.
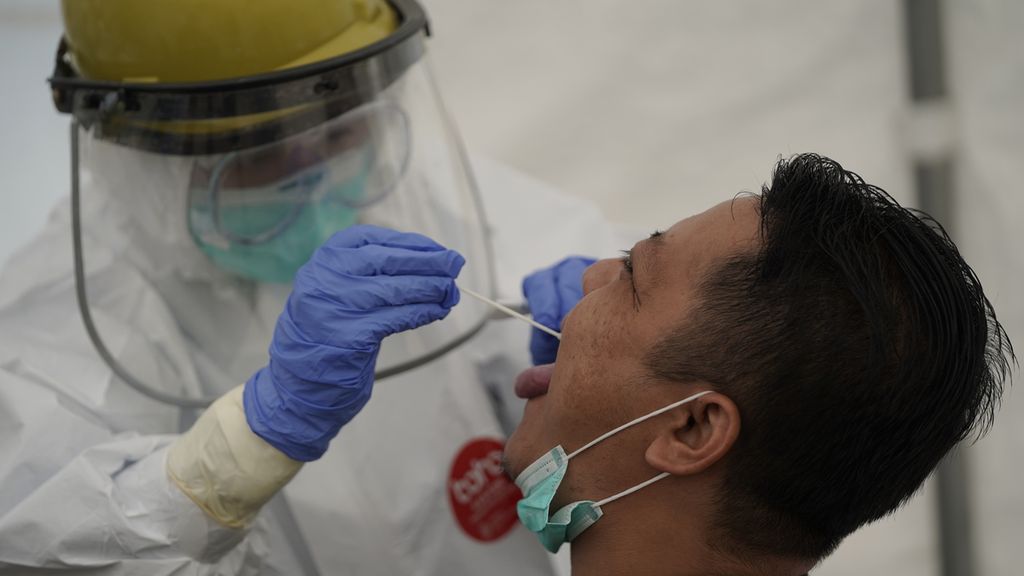
A medical worker takes a saliva sample for a swab test at the Duren Sawit puskesmas (community health center) in East Jakarta on Monday (31/8/2020), when the center tested about 90 local residents. The Indonesian Medical Association (IDI) recorded that 100 doctors had died on the Covid-19 front lines as of Tuesday.
Six months ago, President Joko “Jokowi” Widodo seemed to be racing against time, announcing the first two cases that were confirmed to be infected with the virus that causes COVID-19.
The drums of war against the disease, which at that time had not yet been declared a pandemic by the World Health Organization (WHO), were beaten by the Supreme Commander of Indonesia. A country with the fourth-largest population in the world has the potential to become a fierce battleground against the COVID-19 pandemic.
However, at the beginning of March, people were still astonished to act because the pandemic caused by the previous coronaviruses (SARS and MERS-CoV) had not crossed the Malacca Strait or was still far from Jakarta Bay.
Also read: Hope for the Best, Prepare for the Worst
Only a handful of Indonesians, certainly very old by now, have experienced a series of pandemics in the past. The public was not ready when rats with pestilence were carried in sacks of rice carried by ships to the port of Surabaya, East Java, in 1910. Hundreds of mice then died lying around and rat fleas carrying pestilence transmitted them to humans so that in a short time, there was an explosion of disease.
Pestilence in East Java and Central Java
People made efforts that are irrelevant or even dangerous, such as drinking a tablespoon of kerosene as a measure to prevent pestilence. Disease control through isolation of disease sufferers and blockage of bamboos at home to eliminate rats was done too late. The disease then became endemic to Indonesia, resulting in nearly 250,000 deaths from 1910 to 1960.
There was no effective response to the Spaanse Griep (Spanish flu) pandemic in 1918. The flu quickly spread throughout the Dutch East Indies. Dr. Abdoel Rivai at a meeting at the Dutch Indies People\'s Council accused the Dutch colonial government of being too slow to deal with the Spanish flu pandemic, which resulted in 900,000 people from across the country dying in just four months from August to November 1918.
According to estimates using more sophisticated demographic analysis methods, the death toll during the Spanish flu pandemic was more than 4 million among the 35 million people in Java.
We still remember that in 2009 the swine flu pandemic caused by the H1N1 virus, which was similar to the cause of the Spanish flu. The number of cases reported in Indonesia until September 2009 was nearly 1,100 people, the transmission hit 25 provinces, with 10 deaths.
Also read: The Messages behind the Public Ambiguity
Compare this to COVID-19, which in the two months since the first case was announced, reached nearly 11,000 people from all provinces in Indonesia, with more than 800 deaths. The increase in COVID-19 cases and deaths continues until now — we can no longer stay in the comfort zone.
The battlefield against COVID-19
The general formula for controlling COVID-19 (tracking, checking, and medically treating) is hindered by the development of a polymerase chain reaction (PCR) inspection facility with strict security requirements (biosafety level 2) that takes time to distribute throughout Indonesia.
It is natural for the public to question whether the reported number of COVID-19 cases and death toll is lower than the actual number, due to limited detection of cases and confirmation of deaths due to COVID-19. The number of PCR examinations has indeed increased from day to day, toward the WHO recommendation of 1,000 tests per million population within a week.
Obstacles in PCR examinations do not cover up the reality that should trigger us to work harder. Of the 100 people examined, on average, more than 10 are positive. This figure is still rising from day to day. The PCR examination in Singapore only produces a positive rate of 1.8 percent.

MCoordinating Minister for the Economy who is also chairman of the Covid-19 Control and National Economic Recovery Committee Airlangga Hartarto (two left) witnessed by the Head of the National Disaster Management Agency (BNPB) as well as Chair of the Covid-19 Task Force Doni Monardo (right) campaigning for discipline wearing masks at the main stadium Gelora Bung Karno, Senayan, Jakarta, on Sunday (30/8/2020).
Malaysia once experienced rapid and widespread transmission in all states and was rated as the epicenter. However, the positive rate from PCR examinations in Malaysia is now only 0.1 percent, at a time when Indonesia is trying to slow down the increase, which has already passed 13 percent.
Not ready
At first, the people of Malaysia were not prepared to face the COVID-19 pandemic because they were not sure that the disease was quite dangerous. Meanwhile, there was a political crisis in the country. It was only when the number of cases increased from 99 people (none died yet) on March 8 to more than 1,300 in the next two weeks, with 10 deaths, that panic emerged among the Malaysian public.
Feeling like it was in an emergency situation, the Malaysian government issued a Movement Control Order policy that required people to stay at home, wear masks and keep their distance.
Also read: Protect Oneself and the Surroundings
To meet the needs of personal protective gear and basic necessities, there was a lot of support in the contribution of money and goods by the private sector and community members. Malaysia\'s success story in controlling the COVID-19 pandemic is now one of the role models in the world, along with Taiwan and South Korea.
More than 80 percent of those who infected by COVID-19 only feel a fever, lose their taste and smell, and have muscle aches and light coughs — some even do not feel any symptoms.
Why do people not believe that COVID-19 is dangerous and deadly? Although our eyes and ears almost every day see pictures or hear about coffins in the mass media or social media, our recorded experiences convinced that most of those who are infected by COVID-19 have mild symptoms and are experiencing recovery. More than 80 percent of those who infected by COVID-19 only feel a fever, lose their taste and smell, and have muscle aches and light coughs — some even do not feel any symptoms.
Of the 1,308 participants and teaching staff of the Army Officer Candidate School who tested positive for COVID-19, none were seriously ill or died and now all have been declared cured. Several COVID-19 "patients" were seen to be able to line up firmly and answer aloud questions from the Army’s Chief of Staff.
The COVID-19 infection without causing symptoms is worth praising. On the other hand, what if those without symptoms mingle and have the potential to transmit COVID-19 to those at risk, for example people with obese, diabetes or immune system disorders. Many victims need affordable services from their communities. The role of doctors and officers in community health centers (Puskesmas) or primary care clinics who have been working in silence is very big.
They are tireless, educate the public, protect people with chronic diseases, supervise the quarantine and isolation in homes or field hospitals and become models for preventing COVID-19. Armed with simple medicines, such as aspilet to prevent blood clots, vitamin C, vitamin D and zinc to strengthen the immune system, primary care doctors are doing their best to protect people with COVID-19 virus from getting worse and needing treatment at a hospital.
Also read: The Continuing Struggle of Recovered Covid-19 Patients
Simple laboratory equipment to calculate the absolute and relative numbers of white blood cell types is needed in primary care to detect early symptoms and monitor the course of COVID-19 after being confirmed by PCR examination. Likewise, the pulse oximeter is an important tool for detecting whether a potential COVID-19 patient has a lack of oxygen in the blood. One of the worrying symptoms experienced by people with COVID-19 is a lack of oxygen without showing symptoms (happy hypoxia), where some cases seem like a sudden death.
The clinical skills of doctors in primary care, equipped with limited facilities, can support the decision when a person with COVID-19 can be observed in a field hospital until they are declared to have recovered or must be referred to a hospital with an intensive care facility.
Strategy to fight against COVID-19
Clinical trials to find antiviral drugs in the fight against COVID-19 are hindered by a research replication crisis, with variations in clinical trial results between one research center and another. Prominent drugs in the United States and Europe, such as remdesivir and favipiravir, do not significantly reduce case-fatality.
Residents cross an invitation to fight Covid-19 in the Bukit Duri area, South Jakarta, on Tuesday (1/9/2020).
The use of the lopinavir-ritonavir and hydroxychloroquine drugs, which have sparked debate in Indonesia, is not recommended by WHO, based on the recommendation of the Steering Committee for the Solidarity Trial of COVID-19 drugs for patients who are hospitalized.
Previously, these drugs were used in the US, European countries, the Middle East and others. There is still a possibility of clinical trials of these antiviral drugs for outpatients. The Centers for Disease Control in the US said: "There is no cure for COVID-19 yet.”
In the absence of effective drugs, the world community hopes for a vaccine against COVID-19, some of which are already in the third phase of clinical trials. The government, through Bio Farma and Padjadjaran University, in collaboration with Sinovac Biotech, China, is conducting a third phase clinical trial of a vaccine candidate from an inactivated virus. A potential virus named CoronaVac since July has been used for emergency conditions in China, for example given to health workers.
The Gamaleya Research Center in Russia has also produced a vaccine called Sputnik V, which has been registered as the world\'s first anti-COVID-19 vaccine. Using adenovirus vector technology that can express a portion of the SARS-CoV-2 virus protein to trigger immunity against the virus that causes COVID-19, Sputnik V is likely to seize the largest share of the anti-COVID-19 vaccine market in the world. CoronaVac and Sputnik V are safe for humans, but it will still take several months of observation to determine whether they are able to provide protection from COVID-19.
The SARS-CoV-2 virus that causes COVID-19 is under pressure by the human immune system so that it continues to change to maintain its existence in the world. Mutations found throughout the world, not only in Indonesia, are changes from D614 to G614 (known as D614G), which is the replacement of aspartate acid into glycine at the protein S position at number 614.
The virus that undergoes this change is thought to be more stable, dominating quickly once it reaches an area of infection. It is not known whether the mutation resulted in a more severe COVID-19. It has been investigated that D614G does not change the targets aimed by the vaccines currently undergoing clinical trials.

Cilandak Subdistrict officers wear complete personal protective equipment carrying the Covid-19 coffin after socializing the dangers of Covid-19 in front of a supermarket on Jalan Fatmawati, Cilandak, South Jakarta, on Tuesday (1/9/2020).
The spread of the virus in Indonesia is still quite intensive, the percentage of positive PCR results continues to rise, the highest in Southeast Asia. The health system must rely on primary services under family doctors leading the forces against COVID-19 on the front lines. The principle of combat in primary service follows the strategy of the Sun Tzu War (544-496 BC), "the good warrior places himself in a difficult position to defeat while waiting for the opportunity to destroy the enemy”.
Also read: Curfews in Bogor and Depok Not Effective without Jakarta Following Suit
Do not let COVID-19 patients fall in such a severe condition that they need a ventilator, with the hope that only 15 percent or less survive. Primary services provide protection for those at high risk.
Primordial prevention strategies are a priority, residents of the community should not be exposed to the virus, must avoid red areas, stay away from crowds, and keep their distance. Masks and washing hands as a routine must be supported by a structured environment for daily activities that forces people to behave in adapting to the threat of a pandemic.
The COVID-19 virus can only survive if it finds humans as a shelter for breeding. The fight against COVID-19 will still take months to come. This bitter reality must whip up the enthusiasm to be able to win battle after battle with enemies who use mechanisms in the human body to destroy humans themselves.

Hari Kusnanto Guru Besar Ilmu Kesehatan Masyarakat dan Fakultas Kedokteran Komunitas UGM
It is true that Walt Kelly said in the Pogo comic, "We have found the enemy, it is ourselves". Is it really not easy for us to wear masks outside the home, keep our distance, avoid crowds and wash our hands regularly with soap or sanitizer?
Hari Kusnanto, Professor of the Department of Family and Community Medicine, the School of Medicine, Gadjah Mada University